98217 33877
info.secretarymus@gmail.com-
-
E-7,East of Kailash,
New Delhi -110065 -
Reg.no.
S/1366/Distt.South/2013
27 Jun 2018
News Letter March
From the desk of Gen. Sec MUS
Dear Colleagues,
Musculoskeletal Ultrasound is gradually gaining strength through the support and encouragement from colleagues who have common aims and objectives . Current News letter brings you the vision of one such progressive minded Radiologist Dr. P. Lonikar. We thank him for sharing his insight with the readers and inspiring a deep confidence in the modality and Society.
Open letter to MUS from Dr. Pramod Lonikar, President MSBIRIA, Past Treasurer IRIA
Seasons Greetings!
Recently I came across the work by Muskuloskeletal Ultrasound Society & an idea struck me….to share some insights of mine with the readers.
I congratulate you all for propagating such an innovative & mammoth task.
Since last 10- 15 years, with the technological advancements in Ultrasonography machines- MSK USG has emerged & coursed through many a mile stones. There is maturity in MSK USG usages amongst the clinicians’ & Radiologists’ minds.
Competition is with cross sectional imaging.
To enhance this cause, may I suggest some steps which you might have also thought of, but I am putting them down in words:
1. Need is to increase the popularity of this module percolation to the grass root level availability of cross sectional modalities & cost factor play a major role at this level.. Radiologist is busy with Obstetrics & abdominal part of USG but with PC-PNDT related issues MSK- USG will be a good adjuvant as an exciting learning source & this has to be done with the help of exhaustive mailing list across country which must include Teaching Institutions…rather these institutes should have a special focus so that budding radiologists grow well informed with the module
2.Assurance to the radiologists & treating clinicians along with patients that this is the best, quickest, safest modality we are adopting towards diagnosis & treatment management . Further evaluation with MR or CT should be requisitioned if the clinical suspicion does not match the USG findings. MRI & CT especially 3 D CT are competitors.
3. A special focus should be on USG guided interventions which has plethora of indications & instant satisfaction of clinicians / patients vis-Ã -vis quick result and time saving.
4. Rheumatology is a fast emerging branch in India & use of MSK USG in rheumatology should have a special focus.
5. Readymade teaching modules along with aims & objectives at the end of course expected to be learned by the attendee should be followed up by the teaching faculty. Most of the times we do not know about newer applications & their usefulness which needs to be reinforced.
6. Setting of examination protocols & standardization of reporting.
7. Important issue is data bank of Speakers along with their topics of interests- in this field- a call for speaker names so that interested professionals can access them & invites then to deliver lectures to help this modality flourish.
8. All other stake holders like Orthopedicians, pain management Consultants, rheumatologists, sport medicine physicians, and Rehabilitative Specialists are also to be kept in loop- for that we can have lectures in their clinical meetings, conferences which will have a positive impact in creating a need based usefulness of this modality.
9. Involvement of ICRI, IRIA & its State chapters- keeping in touch with them, offering them teaching courses will also help. Try to have more articles published in various reputed journals including IJRI.
Having tie- ups, affiliation, exchange programs with International societies, who are pioneer in this field will also have positive enhancement of this cause.
As a grass root level foot soldier I agree that suggestions are always better on paper & hard to implement.
I would like to congratulate Dr Rajesh Gothi, Dr Sanjay Thulkar, Dr Nidhi Bhatnagar & all other office bearers for holding the baton & I am sure that under your able leadership MUS will achieve great heights.
Thanks,
With Warms Regards & Best Wishes,
Speaking of confidence building exercise at National and International level , we are very happy to bring the news of our academic affiliation with E.S.S.R (European Society of Skeletal Radiology) and S.U.A (Society of Ultrasound in Anaesthesia), UK
At National level we have been given consent of affiliation by IASM (Indian Association of Sports Medicine ), DOA (Delhi Orthopedic Association) and are working at confidence building exercise with WIP (World Institute of Pain management) and Indian Rheumatology Association.
Our academic activity as CME is being organized on the 12th April on shoulder and knee joint. Interested Consultants may contact MUS at the earliest since we are including only 40 participants. This will be followed by hands- on- workshop in July 2014.
We are today touching upon some basics to lay a strong foundation towards performing quality MSK-USG.
European Society of MusculoSkeletal Radiology Musculoskeletal Ultrasound-- Shoulder
Although patient’s positioning for shoulder US varies widely across different Countries and Institutions reflecting multifaceted opinions and experiences of different examiners, we strongly recommend to examine the patient while seated on a revolving stool. This position allows the examiner to reach the anterior, lateral and posterior aspects of the shoulder with the probe by simply asking the patient to rotate on the chair.
Structures to look for:
Long head of the biceps- Both the intra-articular and extra-articular component
Tendon of Subscapularis and its foot print
Tendon of supraspinatous , foot print and critical zone
Posterior glenoid labrum with infra-spinatous and teres minor
Antero-medial structures and Coraco-acromial ligament
Sub-acromial space and relative configuration of acromion process
Posterior structures with gleno-humeral joint recess
Acromio-clavicular joint
Dynamic scan for impingement
Contours and surfaces of underlying bony landmarks- bicipital groove and greater tuberosity.
How important it is to familiarize one self with the basic techniques and protocols of performing an optimal quality MSK-USG is touched upon by today’s case study.
Case presentation:
A young lady of 26 yrs, of medium build and having Body mass Index within normal range
was referred for ultrasound of the S.I.Joint for the c/o pain of 3-4 months duration.
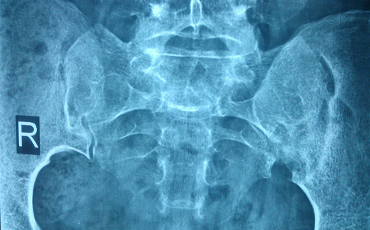
She was carrying a good quality Radiograph of both S.I.Joints AP view Reported Sacroilitis, left side

Also an MRI both S. I. Joints : Reported Sacroilitis Left S.I. Joint .
There was very minimal symptomatic relief after two weeks of treatment with anti-inflammatory drugs . Finally the treating Consultant orthopedician sent her for HFUS of both S.I Joints for evaluation of any additional pathology and assessment for intra-articular steroid injection under ultrasound guidance, if need be .
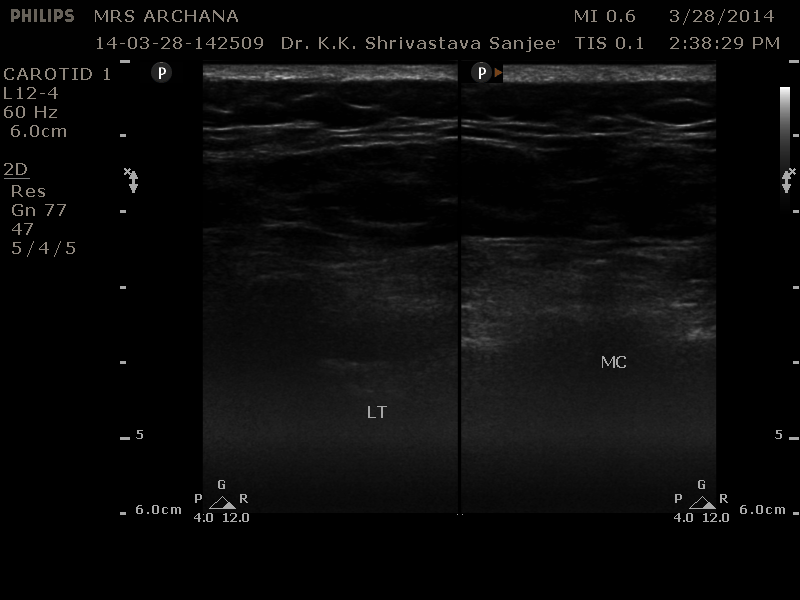
As is the standard protocol, S.I.Joints are evaluated with Linear multifrequency (12-5 Mhz) probe in prone position.
The image obtained shows Skin, SCT ( fat with well defined interfascial septas) Underlying bony land marks of centrally placed median crest and winged out lateral masses bilaterally. As is well appreciated the image is very poor quality and deeper planes are indistinguishable.
Patient was not obese however the fat composition of certain individuals precludes optimal visualization of deeper structures . THI (Tissue harmonics app) works on the similar principles. ref: Investigation on effects of subcutaneous fat on image quality performance of 2 D conventional imaging and tissue harmonic imaging ( Dublin Institute of technology)
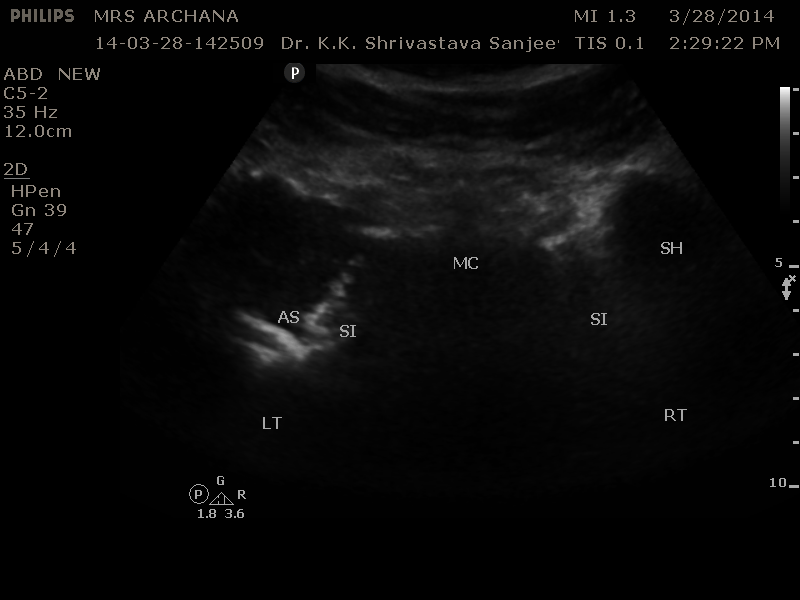
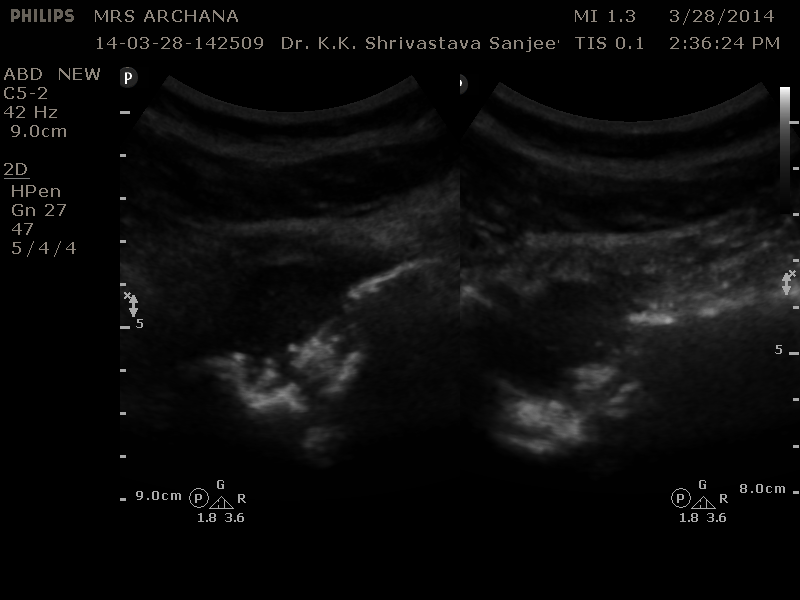
The scan transducer was changed to curvilinear Multifrequency probe ( 5-3 Mhz).
Left S.I. Joint shows altered configuration with underlying cortical destruction of bony land marks as compared to the right side.
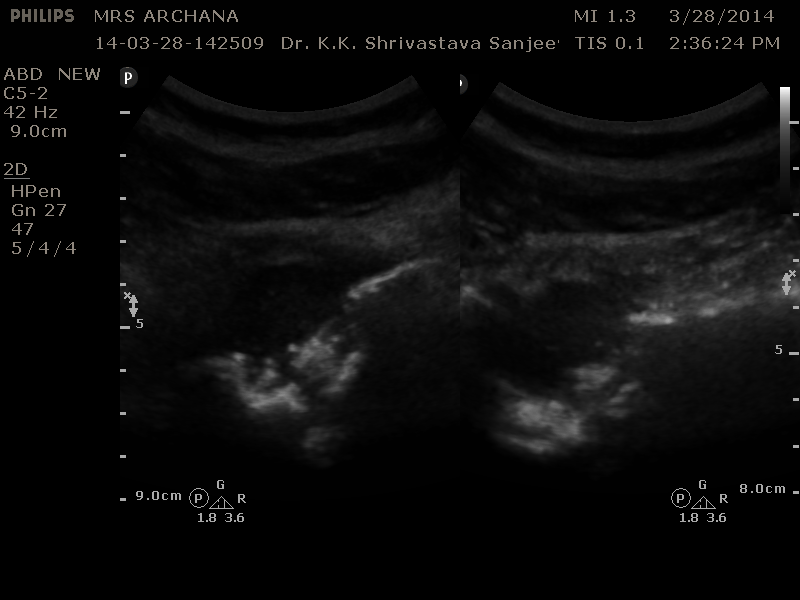
Targeted view of the left S.I. Joint is showing distended capsule with homogenous fluid collection associated with cortical erosion of the sacral and ileum articular surfaces.
Provisional diagnosis of cold abscess secondary to Koch’s Left S.I. Joint was made .
A confirmation by way of FNA for tissue diagnosis was instituted at the same sitting under USG guidance .
Each case study is a strong lesson in MSK-USG, well learnt and shared.