98217 33877
info.secretarymus@gmail.com-
-
E-7,East of Kailash,
New Delhi -110065 -
Reg.no.
S/1366/Distt.South/2013
16 Aug 2018
Newsletter final
From the desk of the Secretary, MUS
Nearly all technological innovations go through the evolutionary history of ‘Can it ?’ to... ‘it can !’. And , it has been no different in the case of Ultrasound as an investigative modality too. Since early 1950’s when ultrasound was introduced to the Medical world , it moved on from strength to strength , gaining the confidence of clinicians world over. But somehow it could not make in roads in the evaluation of Bones and joints ...till now. The reasons could be many fold , objectively speaking , well we all know Bones are impervious to Ultrasound or then sometimes as subjective as a mind set and MRI. Ultrasound is strongly making its presence felt today in the evaluation of Musculoskeletal system . whether it is in the field of Rheumatology (synovial and inflammatory pathologies), orthopaedics ( articular / bones and joints diseases ) , Pain management ( nerves and soft tissues with intra- articular interventional procedures) , Sports medicine ( in sports injury and point- of -care management) or Rehabilitative fields . Ultrasound as a cross-sectional, dynamic, radiation free modality is impressing the clinicians with its wide range of applications .
Any investigative modality if used indiscriminately for any and every patient complaint can go into a disrepute, however, one must make an effort to apply what is available for a more focussed appreciation of the patient complaint. Ultrasound is one such tool which can be used judiciously as the frontline investigation for the purpose of either making a conclusive diagnosis or isolating the region of interest to be targeted by an alternative modality.
Presenting a case to illustrate this logic and we follow it up with Pearls from Dr. Anmol Maria in today’s newsletter.
Case I Patient, 46 years old with swelling in the arm. No history of trauma or procedure. Having mild pain. Duration of history, 3 mothns.

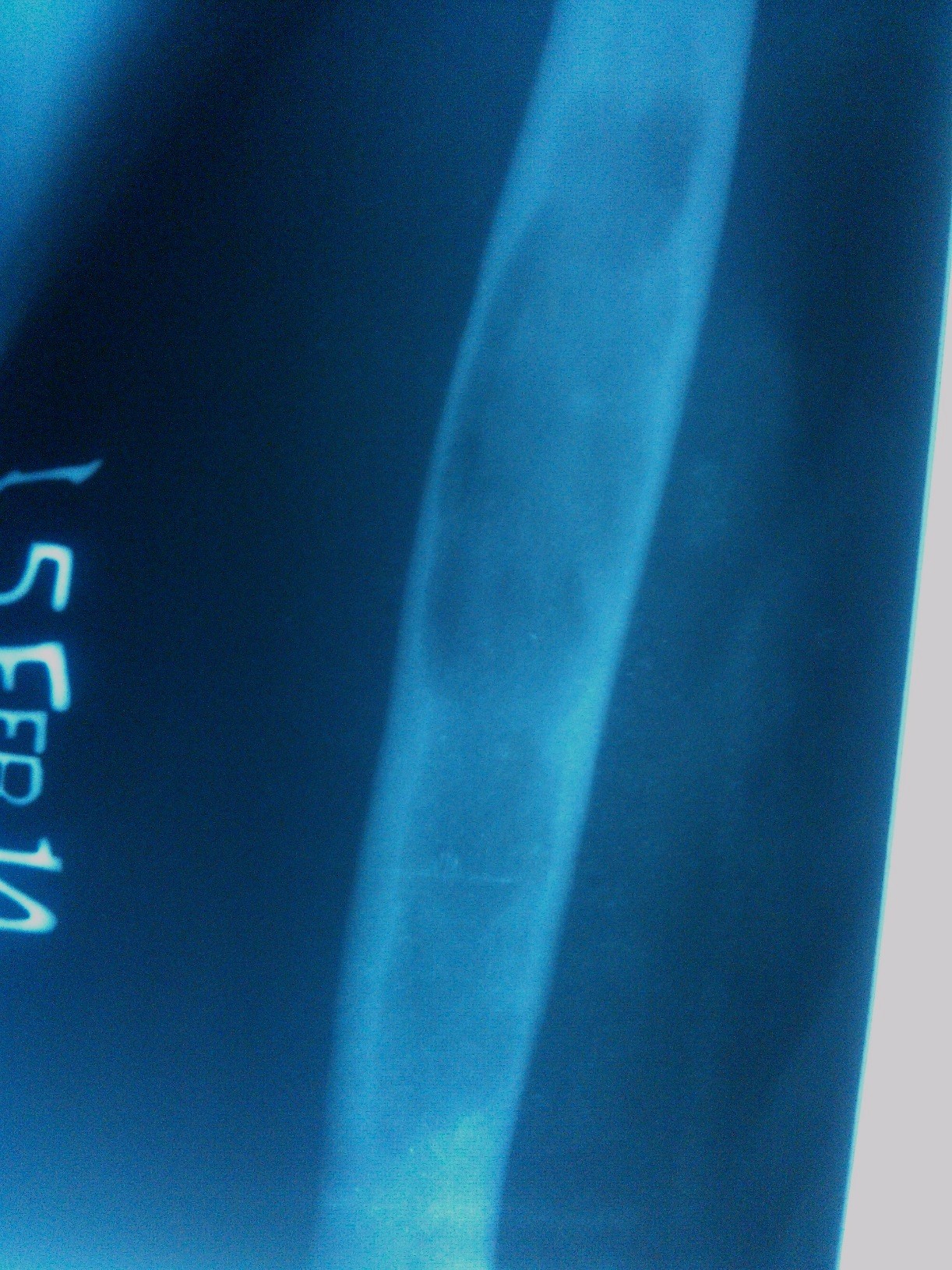
Skigram:AP / Lat views showing expansile medullary radiolucent lesion of shaft humerus with faint septas . No cortical breach, soft tissue swelling +, sparing of metaphyseal region.
Provisional Diagnosis: Fibrous Dysphasia
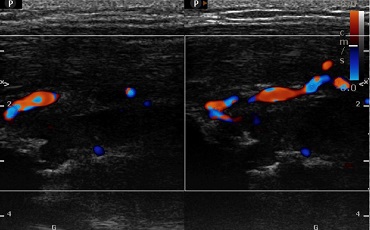
Followed up with HFUS to assess the cause of pain
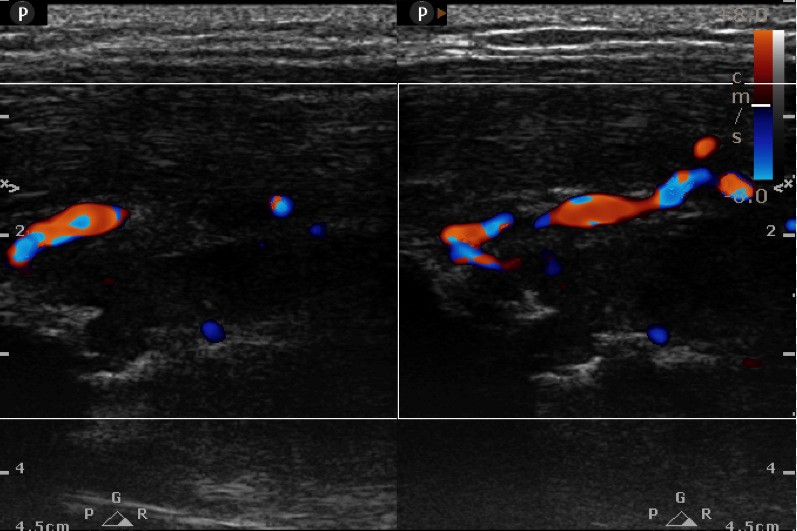
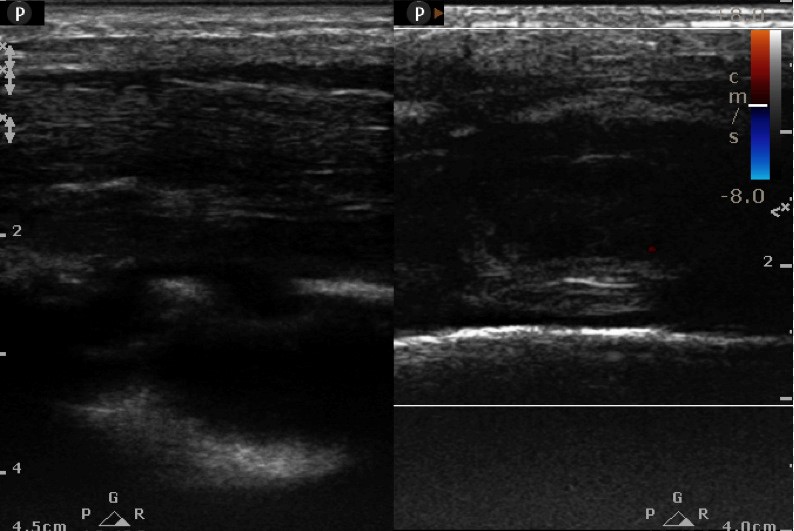
High frequency Ultrasound ( L12-5 MHz) (within 10 minutes of patient skigram): Increased thickness of belly of triceps. On CDU, increase vascularity. Cortical breach as punched - out (*)erosive lesion measuring 4x3 mm in mid shaft posterolateral humerus with new bone formation(^) . No periosteal or juxta cortical fluid.
Ultrasound provisional Diagnosis: Fibroscarcoma. Advised Ultrasound guided Tissue Biopsy.
As directed by the USG findings, further views of the humeral shaft were taken in oblique external rotation to reveal distict cortical thinning along the postero-lateral border, thereby confirming a cortical breach. However, the clinician was not completely convinced and an MRI was requistioned.

Oblique view shows focal area of cortical thinning at the medial border (*)
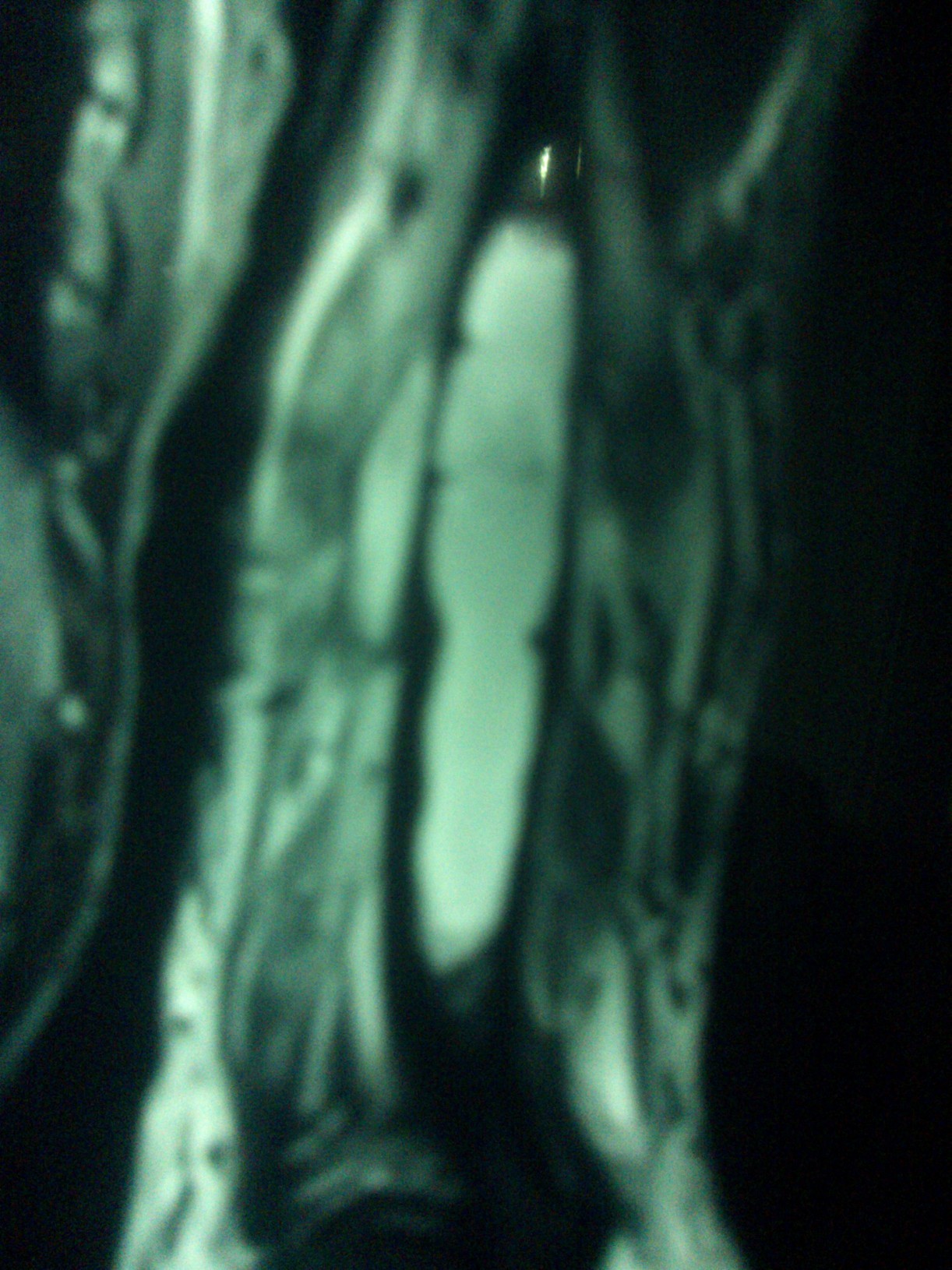
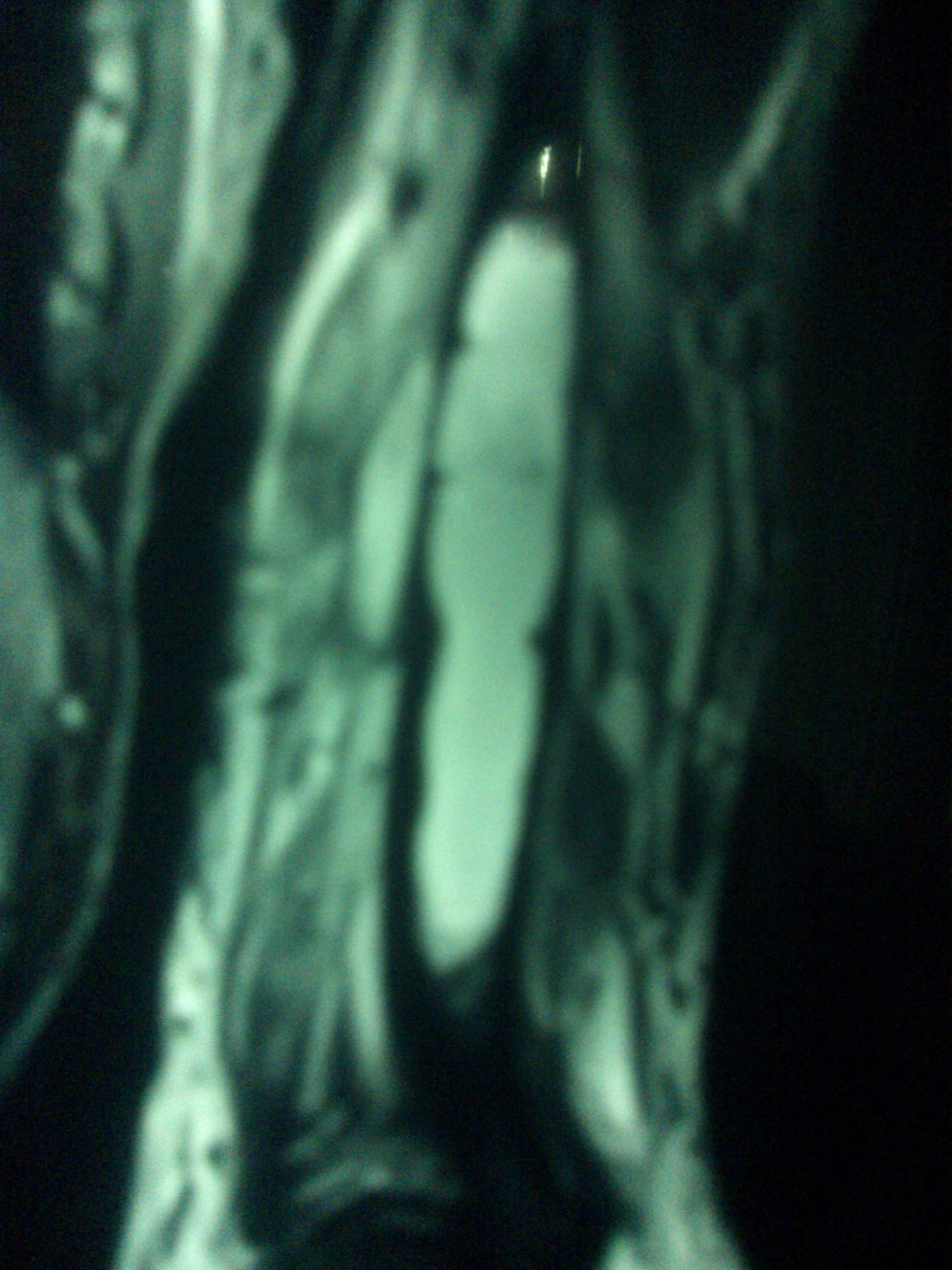
MRI (after 15 days, as patient could not afford it right away): Expansile hypodense lesion with soft tissue mass and cortical thinning of mid shaft humerus.
Diagnosis: ? Osteomyelitis ?? Miotic Lesion
Advised:tissue Biopsy Pateint underwent an open biopsy and findings of malignancy were confirmed on HPE.
Discussion: Could we have saved patient time and money which would have been better utilized for his treatment planning at later stage? Would an ultrasound guided / open biopsy on ultrasound report itself been a QUICKER logical decision ?
Your comments are welcome.